Naming an Unrecognized Type of Abuse in Compulsive Sexual Behavior and Infidelity
This article focuses on naming the dishonesty and deception problem that exists when a person creates and then maintains a deceptive, compartmentalized, sexual or relational reality in the content of intimate partnership or a family system, referred to as deceptive sexuality. Whenever an individual intentionally conceals a deceptive reality from those targeted, they engage in deceptive compartmentalization. This involves subjecting people and relationships to ongoing patterns of dishonesty, deception, and psychological manipulation by intentionally withholding vital, often life-altering information for as long as the secret reality is maintained. This type of behavior inflicts significant harm on individuals and deteriorates the very fabric of relationships.
This article aims to highlight a universally understood but often unspoken truth: dishonesty inflicts profound harm on individuals, relationships, and human life. Subjecting people to patterns of dishonesty and intentionally manipulating their reality through deliberate deception is a form of psychological abuse.
Deceptive Compartmentalization Relies on Integrity Abuse
Engaging in problematic sexual or relational behavior presents one set of issues, but choosing to conceal such behavior introduces additional problems related to integrity, honesty, and the approach one takes in dealing with their problematic behavior towards others in their life. This decision to maintain a deceptive compartmentalization of one’s life—where one part of reality is actively hidden from view and separated from the acknowledged reality—constitutes the crux of what is often a covert psychological operation. This operation aims to keep these dual realities separate, ensuring that those targeted remain unaware of the hidden truth through deliberate deception and intentional manipulation of information. This is akin to military psychological operations, where specific tactics are deployed to manipulate targets’ perception of reality, their emotions, and ultimately their behaviors, to control and exert power.
This concept of deceptive compartmentalization is aptly illustrated by the metaphor of a “secret sexual basement” beneath the “relational home” upstairs, helping to differentiate between the issues of sexual behavior and dishonesty. However, deceptive compartmentalization isn’t limited to sexual misconduct but can also extend to secret financial dealings, substance abuse, or even political maneuvers. Such realities all represent forms of integrity abuse, characterizing what may be termed as integrity-abuse disorder – a condition where dishonest and deceptive behaviors cause significant harm to relationships, be it within intimate partnerships, families, teams, or even larger social or national collective relating.
Explaining Integrity Abuse
Here, integrity is defined as honesty. The dishonest, deceptive, and manipulative behaviors associated with deceptive compartmentalization, act as patterns in a relationship, and are identified here as, integrity abuse.
All humans exhibit integrity deficits to some extent, and integrity should not be viewed in absolute terms. An integrity disorder, or integrity-abuse disorder, emerges when an individual’s dishonesty reaches a level that significantly impacts their own life or causes substantial harm to others and their relationships. This term links dishonest behaviors to their harmful impacts, especially when they lead to psychological, emotional, and relational injury and distress. When these behaviors result in significant distress and impair life functioning, the situation escalates into what may be classified clinically as an integrity-abuse disorder.
An integrity-abuse disorder manifests through persistent dishonesty, becoming abusive when it actively harms others through deceit, omission, systemic gaslighting, and other detrimental behaviors driven by an agenda of deception. This article focuses on the term “integrity-abuse disorder” to broaden our understanding of this form of maltreatment, particularly as it relates to secretive sexual behaviors and deceptive sexuality. The goal is to explore how such disorders affect human relationships and the broader implications for those involved.
Integrity-Abuse Disorder
Integrity-abuse disorder (IAD) is a clinical term for a type of conduct disorder. IAD manifests through dishonesty and deception that damages relationships and exploits others for personal gain, often based on an agenda of maintaining power and control, avoiding accountability, and compartmentalizing a hidden reality through deliberate deception. IAD involves both overt and covert strategies to dominate and manipulate, extending from intimate relationships to broader social interactions.
Key behaviors and Characteristics of IAD include:
- Persistent violation of others’ rights
- A lack of empathy for others’ feelings and situations
- Consistent engagement in deceitful behavior to mislead or trick others
- Intentionally manipulating a person’s reality
- Manipulation of facts and situations to benefit oneself at the expense of others
- Utilizing charm, seduction, or intimidation to exploit individuals for personal benefit
- Showing a disregard for moral standards, integrity, honest, or just behavior or treatment of human beings
- Engaging in impulsive and reckless behavior that can endanger social or personal relationships
- Exhibiting a lack of remorse for harm caused, coupled with indifferent or callous attitudes towards those affected.
- Tendency to shift blame and responsibility onto others to avoid accountability
- Using defensive maneuvers that compromise ethical standards
- Employing coercive tactics to control or manipulate others
Although isolated incidents of dishonesty and integrity deficits are not uncommon, consistent engagement in these behaviors that subject others to psychological, emotional, and relational harm constitutes a form of intimate partner abuse, psychological abuse, and domestic maltreatment, thereby defining a pattern of sociopathic behavior known as IAD. When individuals are repeatedly subjected to such patterns of harm, particularly when they lack viable escape routes or are in a state of disempowerment, they are at risk of developing complex trauma symptoms.
Have we forgotten that honesty is essential to human and relational health?
An Example of Integrity Abuse
Imagine that you own a 30-year-old business with two other business partners. Now imagine that your two business partners were scheming together the whole time, stealing hundreds of thousands of dollars from you – manipulating you the whole time without your knowledge at all. Consider that you felt very close to them for the entire 30 years of the business. You had deep respect for them, many good times together, and a deep sense of loyalty to the business. Your discovery of the scheming and manipulating has taken you completely by surprise and has felt like a jarring shock to your system and your sense of reality.
The Three Phases of Deceptive Sexuality Integrity-Abuse Disorder
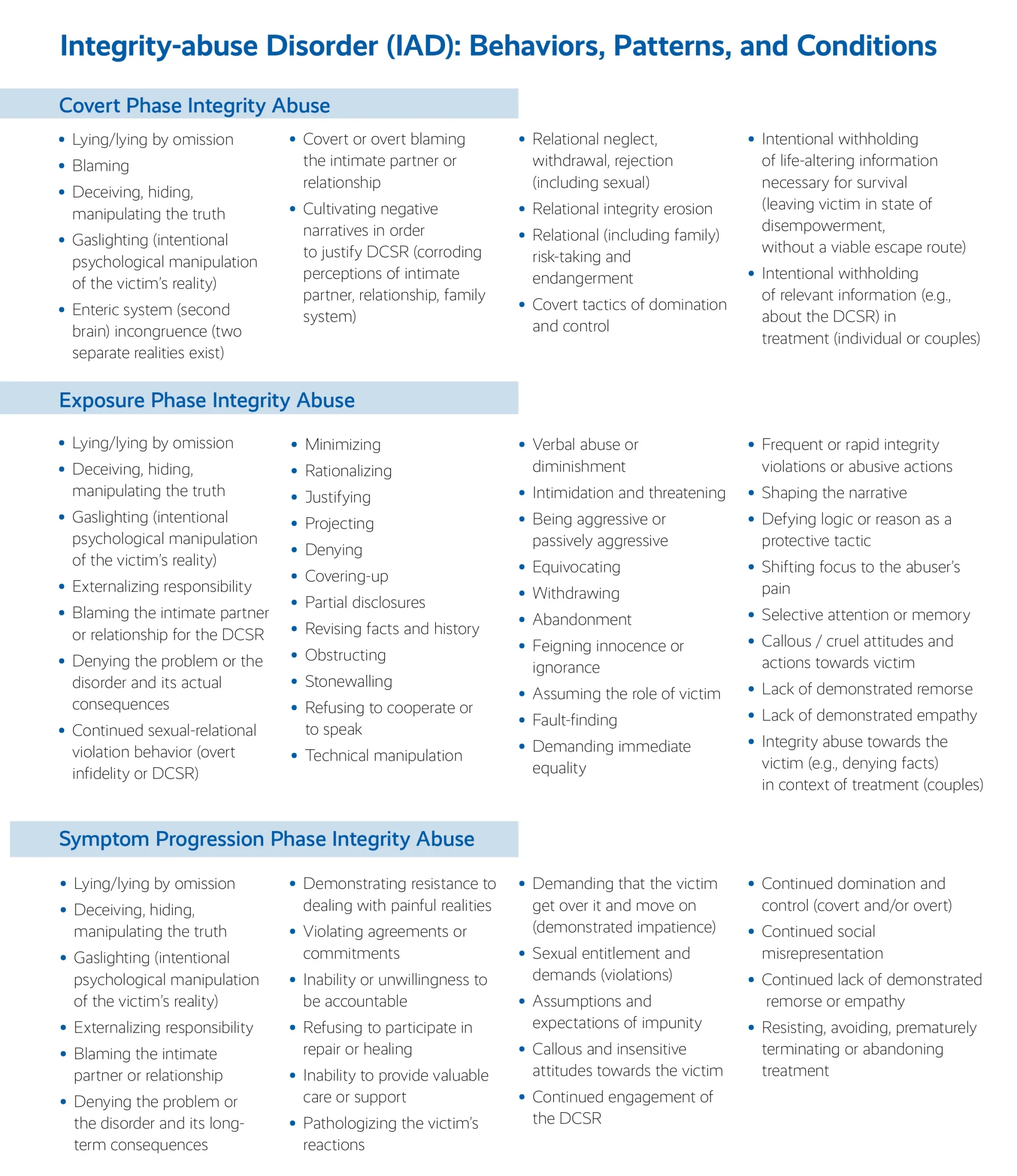
Now, let’s focus on deceptive sexuality and the integrity-abuse disorder involved when there is a secret sexual life being deceptively hidden. In this model of abuse and trauma, the traumatic impacts manifest through a sequence of three distinct phases, each characterized by specific behaviors and consequences that compound the psychological, emotional, and relational trauma experienced by victims. Each phase involves integrity-abuse behaviors and tactics being used by the abuser, as well as description of the conditions that may exists, which are also harmful.
As IAD progresses through its distinct phases – Covert, Exposure, and Symptom Progression – each stage intensifies the psychological, emotional, and relational trauma experienced by victims. Initially, victims are manipulated without their knowledge, leading to disempowerment and vulnerability. As the abuse becomes apparent, the traumatic exposure disrupts their sense of reality, compounding their distress. Even after discovery, the manipulation often doesn’t cease; it may escalate, become overt, or may eventually become more subtle and psychologically complex, leading to long-term damage. The term, DCSR, refers to the deceptive, compartmentalized, sexual or relational reality, otherwise referred to metaphorically as the secret sexual basement.
1. Covert Phase
In any situation involving deceptive compartmentalization, there is an initial phase where reality is actively concealed. During this phase, the victims are unaware of the manipulation they’re undergoing, and their perception of reality is manipulated and controlled by the person orchestrating the deception. In addition, there are many other types of destructive behaviors and conditions that occur during the covert phase that have notable consequences. Indeed, once a deceptive reality is created, it requires an ongoing system of management that includes behaviors that are used to keep the basement hidden. Strategies are carried out to hide truths, cover tracks, and manipulate people and situations in order to keep the DCSR from being discovered. This is the covert phase.
Covert Phase Integrity-abuse Behaviors
Some of the most common deceptive and defensive tactics (or integrity-abuse behaviors) that perpetrators use during the covert phase to protect and maintain a secret sexual life include:
- Gaslighting. Gaslighting during the covert phase refers to abusers’ intentionally manipulating their partners’ realities (PRE) to keep the secret reality hidden (Dorpat, 1994; Dorpat, 1996; Gass, 1988; Jason, 2009). Abusers that actively gaslight redirect and distort their partner’s reality to keep the sexual basement secret. Examples of active gaslighting behaviors include excuses for being late from work, lies about having to stay on a business trip for an extra day, etc. Passive gaslighting refers to the presence of an unknown reality and considerable threat on an ongoing basis.
- Lying outright, lying by omission, or telling partial truths. Lying or telling partial truths can seriously impact trust, reliance, attachment, and intimacy in a relationship (even if the lying or partial truth telling is “perceived” only at a deeply unconscious level).
- Manipulating relational states. Sometimes the abuser will create specific states in the relationship for reasons that may have to do with the DCSR (e.g., suggesting that the wife looks tired so she may go to bed early and leave him the opportunity to have webcam sex with a person online; starting a fight to create a reason to leave home and engage in the DCSR). By creating these states, the abuser effectively creates self-doubt and self-blame in the partner as a way to get her preoccupied with her deficits. If she is preoccupied in this way, she is less likely to confront him or his deceptive behavior.
- Using threats, anger, and intimidation to maintain control and power. The abuser may use subtle or overt forms of abandonment threats, financial threats, anger, and/or intimidation to keep their partner from inquiring about or discovering the secret basement.
- Shaming and finding fault. Abusers may use shaming and finding faults in their partner as a way to create self-doubt in the partner and to keep the deceptive sexual reality hidden.
- Externalizing responsibility and victim-blaming. As relational problems and family symptoms emerge, the abuser may try to avoid responsibility by intentionally externalizing blame to the partner, the relationship, or other factors. People who engage in secret sexual lives often need some sort of justification or rationalization to continue developing and maintaining their hidden worlds. It’s just much “easier” to engage in deceitful and hurtful behaviors if you perceive the “fault” as stemming from the person that you’re hurting.
Covert Phase Integrity-abuse Conditions
The creation and existence of a secret sexual life leads to abusive conditions, which set up a reality that is potentially abusive, oppressive, and harmful. The person who created the secret sexual basement often develops a thought system that minimizes, justifies, rationalizes, denies, and/or defends their hidden reality. This, in turn, negatively impacts how the abuser perceives and interacts with their intimate partner and the relationship, likely for many years to come. Common abusive conditions that occur during the covert phase include:
- Relational withdrawal and neglect. Creating and maintaining a DCSR while in an intimate partnership often takes away time, energy, attention, intimacy, emotions, and even financial investment from the relationship. As a result, the partner who is unaware of what is going on is left without the attention and nurturing that they deserve. On top of this, they are likely to feel confused and anxious as to why their partner is withdrawn and unavailable.
- Endangerment. Deceptive sexual realities are often associated with serious and potentially life-threatening risks, both for the abusers and the unknowing partners, as well as their loved ones and family members (e.g., engaging in unprotected sex that goes uncommunicated; the creation of situations that could lead to other individuals’ vengeful violence or retributive behaviors such as stalking or acting out on social media). Secret sexual lives ultimately create the risk of eventual separation or divorce. Each of these risks is associated with heightened potential for negative and traumatic experiences that will impact all persons involved in the relationship.
- Covert dominance and control. During the covert phase, abusers tend to have a significant amount of covert power and control over their partners. By withholding life-altering information from their partners, they effectively strip away their partners’ ability to truly understand key aspects of their intimate relationships, along with the power to make healthy, self-protective decisions. Abusers who hold sexual secrets prevent their partners from acting based on reality, and ultimately keep them paralyzed, and being held hostage, in a destructive pattern of uninformed immobility or chronic disempowerment.
- Lack of informed consent. Many partners in these situations engage in intimacy with the abusers without knowledge about the deceptive reality. In such cases, these partners are not consenting to intimacy based on complete information about the abuser and their deceptive sexual realities. Partners may even make life-altering decisions without full awareness of the truth (e.g., to have a child). Partners in these situations are robbed of the option to make fully informed decisions about and to provide fully informed consent related to their lives.
- Breach of relationship agreements. Involvement in a deceptive reality violates the primary relationship’s agreement or contract related to sexual and/or emotional monogamy. Consider how this shape the abuser’s perceptions of and feelings toward their partner, as well as the degree of investment they have for the relationship. Consider how an unknowing person living with a DCSR may react, at a gut instinct level, to living with ongoing sexual or romantic infidelities.
Subjecting people to patterns of dishonesty and intentionally manipulating their reality through deliberate deception is a form of psychological and relational abuse.
- Dehumanization. Abusers often need to compartmentalize, to an extreme degree, their feelings about themselves, their partners, and their family members. At some point, most abusers need to cognitively render their partners/ family members as less important than the secret sexual basement. This deprioritization leads to the dehumanization of people who are cared for and loved by the abuser.
- Sexual entitlement over human rights. A secret sexual basement creates a condition where sexual entitlement is prioritized over the basic human rights of those who are being deceived. For the abuser, it is more important to create and maintain the DCSR than it is to allow people to know the truth so that they can make basic, informed life choices. Masculinity socialization includes the belief that creating and maintaining a secret sexual life is part of masculine power and privilege, and boys and men are groomed to deal with life by taking advantage of this form of sexual entitlement. Further, men often may still consider a man with a dishonest sexual life as a “man of integrity”, and he may actually gain masculinity status by having a secret sexual life.
- Social misrepresentation. During the covert phase, the abuser might misrepresent their partner and the relationship. For example, they might communicate to others that the relationship is not monogamous (even when the partner believes that it is). They might lie and manipulate other people into believing that they have a hopelessly unhappy relationship, that they are almost divorced, or that they are single. As such, they might gain the trust and support of other people who unknowingly provide encouragement for the DCSR.
- Social collusion. During the covert phase, other people may know about the secret sexual reality (e.g., a neighbor, friend, relative or coworker; or within corporate, military, community, or sports contexts) and intentionally withhold important information from the victim. To the victim, this can be experienced as a form of social collusion against themselves, their children, and their family. The victim may experience it as a sort of community-level violation or betrayal that leads to short- and long-term emotional and psychological injury.
2. Exposure Phase
This phase involves when the abuser is confronted, particularly with the revelation of the covert reality and the associated behaviors and manipulations. When individuals engage in deceptive compartmentalization, their victims may eventually begin to sense inconsistencies, leading them to question, challenge, or confront the abuser. This often culminates in a critical moment or period when those being deceived and psychologically manipulated uncover the ongoing, systematic deception. This marks the beginning of the exposure phase, where the victims become fully aware of the truth – that they have been systematically lied to and that a hidden reality has been deliberately concealed from them, sometimes for decades.
During the exposure phase, victims often experience intense, ongoing integrity abuse in the form of continuing patterns of emotional, psychological, and relational harm. The discovery of such a profound and intense deceptive reality, particularly one involving sexual or relational elements, can shatter the survivors’ entire sense of self, identity, and understanding of their intimate relationships, marriage, and family. This type of revelation fundamentally alters their reality, often resulting in a global injury that reshapes their future and that of their children.
The discovery and exposure to the intense and deceptive reality of sexual and relational compartmentalization can shatter and substantially demolish a survivor’s entire construct of self, identity, intimate relationships, and family, altering their lives and futures to the point of global injury. This experience amounts to a psychological and relational death experience, where it becomes impossible to recreate the pre-exposure reality (PRE) in its original form. While humans can adapt and reconstruct their egos and realities, the original PRE cannot be fully restored, leading to a significant psychological and relational loss. This loss necessitates a complex and unique trauma and grief process, often unrecognized and illegitimatized by society and institutions, leaving those affected by this reality-ego fragmentation (REF) with a profound and unrecognized psychological injury.
Exposure Phase Integrity-Abuse Behaviors
After the discovery of the deception, the person with the IAD will often try to defend themselves and to protect the truth from being exposed by utilizing specific defenses. Some of the most common types of integrity-abuse behaviors that occur during the exposure phase include:
- Denial and obstruction. Some abusers will overtly deny the existence of the sexual or relational truth by stonewalling, refusing to speak or listen to their partners, lying, using cover-up narratives, and/or destroying or hiding evidence. Many will attempt to minimize the nature, frequency, duration, and/or content of the behaviors as well as the intention and meaning of the behaviors. Abusers will often try to deny how significant and impactful the discovery of this sexual reality is to the victim.
- Defensive distortions. Defensive distortions refer to the ways that abusers twist and manipulate reality into different configurations in an attempt to shape victims’ perceptions of truth. For example, minimization may be used to try to make things seem less significant or meaningful than they actually are (e.g., the frequency of sexual behaviors was lower than it really was or that the affair “meant nothing”). Rationalizing and justifying are additional forms of defensive distortions that are also common during the exposure phase.
- Psychological manipulation and gaslighting. Feigning ignorance, confusion, or innocence and pretending to not recall or remember are tactics that might be used to manipulate victims during the exposure phase. Psychological manipulation such as countering and correcting might be used to defend against actual responsibility-taking, to avoid confrontation of the truth, and to create self-doubt in victims.
- Lying or lying by omission. Lying (i.e., overtly lying, lying by omission, and intentionally holding back information that is clearly relevant) is another common integrity-abuse behavior. In fact, some abusers will continue to lie even when there is hard evidence to contradict their inaccurate version of reality. Some abusers might only admit to what the victim already knows and continue to hide the rest. These abusers will often attempt to determine how much is necessary to share, and what can remain deceptively compartmentalized. They will present false, staggered, or partial disclosures as full disclosures and continue their control and domination over their victims by withholding the complete reality. Lying injures trust, violates the victims’ right to the truth and robs the relationship of its relational integrity.
- Externalizing blame and victim blaming. If the deceptive reality is unable to be completely withheld, defenses such as externalizing blame and victim blaming may emerge. Blame might also be assigned to work, stress, other people, drugs, alcohol, etc. More often, however, the intimate partner or the relationship itself become the targets of blame and are cast as at least partly responsible for the deceptive compartmentalization. Sometimes an intimate partner’s body or their lack of sexuality, affection, or attention will be used to justify the secret life. Oftentimes, victims’ symptoms that developed during the covert phase are used by abusers as justification for victim blaming during the exposure phase. This often leads to direct attacks, fault finding, and/or attempts to create self-doubt, guilt, or shame in the victim.
- Domination, power, and control tactics. During the exposure phase, abusers will often express anger and rage at having been caught and/or confronted. Abusers may become verbally abusive, using tactics such as belittling, patronizing, and chronically diminishing. Abusers may also use passive-aggressive threats, violence or the threat of violence, and other forms of domination to control, silence, suppress, and oppress their traumatized partners. Withdrawal or threats of abandonment, including financial abandonment or removal of basic financial support, may be used to manipulate victims or to maintain power over them and to stay in control.
- Continued engagement in the deceptive agenda. Some abusers may continue to engage in the secret sexual basement and to hide, lie, and manipulate even after their partners have been exposed to the previously secret reality. Despite the injury, trauma, and pain experienced by the victims during the exposure phase, some abusers’ sense of entitlement will prevail in these situations, and the deceptive sexual life continues. The abusers in these situations may have promised to stop their compulsive-entitled sexual behaviors; however, at some point they return to their secret basements and re-engage in deception. This sets up the situation for yet another discovery/disclosure and reality fragmentation process.
Exposure Phase Integrity-Abuse Conditions
Integrity abuse during the exposure phase is conceptualized as not only abusive behaviors or conduct, but also as the following abusive conditions or states of being:
- Integrity-abuse bombardment and flooding. During the exposure phase, the frequent and intense integrity-abuse behaviors described previously often overwhelm victims, leaving them unable to prevent, stop, or cope effectively with the onslaught. This relentless exposure to abuse becomes an injurious condition in itself, as victims are bombarded with no time or space to process or metabolize the trauma. The continuous barrage of shocking events prevents the use of healthy coping mechanisms, contributing to a complex trauma shaping process. This adversely affects the victims’ emotional, cognitive, and relational systems, and the harm intensifies with the duration, frequency, and severity of the abuse.
- Avoidance of responsibility. Effective coping and healing begin with identifying the problem and its source, crucially requiring the source (person) to acknowledge their role in the issue. If the source fails to accept responsibility, often denying or misunderstanding the situation, it compounds the victims’ challenges. Consequently, victims are driven to ensure the problem is clearly identified and that the deceptive partners take ownership. However, this process is typically protracted and marred by harmful behaviors, such as defensiveness and escalating deceptive, manipulative, and abusive actions, before abusers finally assume responsibility.
- Lack of detailed disclosure about the DCSR. During the exposure phase, it is not uncommon for abusers to deny the victims access to the reality of the DCSR, despite how important it is that they gain a truthful, accurate, and full clear disclosure. For intimate partners, being prevented from access to this information can be an excruciating and harmful experience to which they may respond with anxiety, anger, and rage. This can often create intense additional injury, trauma activation, and stress for the victims. Indeed, every moment that passes during which the victims are denied crucial information about the DCSR takes them farther away from embarking on their healing processes.
Naming dishonesty as harmful to human beings and human life is imperative in reducing this form of harm and psychological suffering and helps to improve our collective societal health and well-being.
- Protection of self over others. Many of the behaviors that occur during the exposure phase communicate to others that abusers value themselves over their partners and family members. Rather than responding to their victims’ need for important information as a step to treatment and healing, abusers will instead often choose to defend the deceptive compartment and themselves. This often creates an injurious dynamic for the intimate partners, which can lead to high levels of fear, anxiety, anger, and rage.
- Lack of space for partner’s pain. The abuser’s state of mind and inability to face the reality of the situation may result in a lack of space for and appreciation of their partner’s pain. Indeed, the abuser may even sometimes show intolerance towards the intimate partner’s symptoms and may become abusive if the symptoms are expressed in his or her presence.
- Domination and oppression. During the exposure phase, victims are often not allowed to express or to sort through the extreme pain they feel. They are not given the chance to tend to their needs and to start their healing processes. Sometimes abusers dictate what emotional and behavioral reactions and expressions are allowed by their victims. Victims in these types of situations often feel hopelessly deprioritized, dominated, disempowered, and oppressed.
- Inability to provide valuable care and support. If abusers do not take ownership, remain in denial, and/or lack basic comprehension about the problem, then it is unlikely that they will respond to their victims in ways that are healthy and helpful. In these situations, they are unable to act in ways that would help put the traumatic dynamic and process on a path towards recovery and health, repair, and healing. Abusers in this situation are often not able to provide the safety, emergency care and protection, or health-promoting support that would be so beneficial for their partners and families.
- Demand for immediate equality. Abusers will often deny or lack awareness about the impact, intensity, or injuriousness of the situation. In fact, they will often act as if nothing is wrong and expect to be treated as they were before the exposure. They may demand immediate relational equality, sometimes attempting to get it through control, domination, or abuse (e.g., demands for sex or other expectations that are unhealthy and/or abusive). Insistence on immediate relational equality suggests that the abuser does not truly recognize and take responsibility for the level of injury that they have created.
- Social misrepresentation. There may be instances where both the abuser and the victim collaboratively shape the narrative about their relationship and the hidden sexual life to family or community members, aiming to protect the family unit or minimize impact on children. However, conflicts often arise regarding what details to share, with whom, and how. Additionally, there are situations where the abuser unilaterally manipulates the narrative, controlling and dictating the story, thus inflicting further social-level abuse. In such cases, the abuser may determine the specifics of what is shared with others, including children, family, friends, and the broader community, often presenting distorted versions of their partners, relationships, or family dynamics that foster misleading social perceptions and deeply harm victims.
3. Symptom Progression Phase
When abusers are caught and exposed, this does not necessarily mean that the integrity abuse stops. Symptom progression phase integrity-abuse shaping refers to the integrity abuse that occurs during the symptom progression phase: the short-term and long-term impacts and symptoms that occur in the aftermath of the covert and exposure phases.
Symptom Progression Phase Integrity-Abuse Behaviors
- Violations of agreements or commitments
- Inability or unwillingness to be accountable
- Refusal to participate in repair or healing processes
- Inability or unwillingness to provide valuable care and support
- Continued psychological manipulation and gaslighting
- Persistent negative relational patterns and learned helplessness
Symptom Progression Phase Integrity-Abuse Conditions
These continued abusive behaviors often cause victims to suffer from conditions such as:
- Dissociation and numbing
- Compartmentalization
- Denial/normalization
- Reality and ego confusion and instability
- Chronic anxiety and/or depressive disorders
- Physical body and medical symptoms
- Persistent negative relational patterns
- Learned helplessness
- Loss of faith in humanity
Victims in these situations are likely to experience ongoing symptoms related to second brain injury and enteric system confusion (i.e., an inability to be aware of and to effectively respond to one’s “gut instincts”). These individuals may report an ongoing sense of confusion as well as being unsure of what to believe in or what is real. Sometimes, the abuser may re-engage in deception during this phase, thus overlapping a new covert phase with the existing symptom progression phase. This compounds trauma and injuries, adding more complexity and severity to symptoms and additional harm to those involved.
Treatment Implications
This article aimed to highlight a universally understood but often unspoken truth: dishonesty inflicts profound harm on individuals, relationships, and human life. Subjecting people to patterns of dishonesty and intentionally manipulating their reality through deliberate deception is a form of psychological and relational abuse.
Despite considerable professional attention to the treatment for infidelity and problem sexual behavior over the past several decades, an awareness, recognition, or any meaningful integration of the psychological abuse disorder within the framework of infidelity, sex addiction, or compulsive sexual behavior remains a glaring blind-spot, which is also reflected within society at large. So, here we reviewed in three phases, the specific abusive and harmful behaviors and conditions, or the integrity-abuse, related to deceptive sexuality, referring to maintaining a deceptive, compartmentalized sexual or relational reality, while in an intimate partnership or family system.
Introducing and helping patients recognize and identify these integrity-abuse behaviors and conditions seems to be instrumental and profoundly helpful in reducing this type of harm in the author’s experience in clinical practice. It also makes sense, that if as professionals we omit, ignore, or render these behaviors, patterns, and conditions as not even worthy of a name, or bringing attention to, then patients may not be able to address or find relief from this type of harm and suffering. And of course, it is our ethical and professional role and purpose as psychologists and treatment providers to attempt to alleviate human suffering.
Hence, it is important to continue to foster ongoing research, professional and psychological understanding, and then to foster appropriate treatment interventions for integrity-abuse disorder, in and outside of deceptive sexuality, which is simply one area of life where integrity-abuse may occur. It is critical for professionals to start naming this type of human maltreatment.